




Perfect Sight Without Glasses
by William H. Bates, M. D. Д. Бейтс
PERFECT SIGHT WITHOUT GLASSES
CHAPTER XXII
SQUINT AND AMBLYOPIA: THEIR CURE
THE evidence is conclusive that squint and amblyopia, like errors of refraction, are purely functional troubles; and since they are always relieved by the relief of the strain with which they are associated, it follows that any of the methods which promote relaxation and central fixation may be employed for their cure. As in the case of errors of refraction, the squint disappears and the amblyopia is corrected just as soon as the patient gains sufficient mental control to remember a perfectly black period. In this way both conditions can be temporarily relieved in a few seconds, their permanent cure being a mere matter of making this temporary state permanent.
One of the best ways of gaining mental control in cases of squint is to learn how to increase the squint, or produce other kinds of squint, voluntarily. In the case illustrated the patient had divergent vertical squint in both eyes. When the left eye was straight the right eye turned out and up, and when the right eye was straight the left eye turned down and out. Both eyes were amblyopic and there was double vision, with the images sometimes on the same side and sometimes on opposite sides. The patient suffered from headaches, and having obtained no relief from glasses, or other methods of treatment, she made up her mind to an operation and consulted Dr. Gudmund J. Gislason, of Grand Forks, N. D., with a view to having one performed. Dr. Gislason, puzzled to find so many muscles apparently at fault, asked my opinion as to which of them should be operated upon. I showed the patient how to make her squint worse, and recommended that Dr. Gislason treat her by eye education without an operation. He did so, and in less than a month the patient had learned to turn both eyes in voluntarily. At first she did this by looking at a pencil held over the bridge of the nose; but later she became able to do it without the pencil, and ultimately she became able to produce every kind of squint at will. The treatment was not pleasant for her, because the production of new kinds of squint, or the making worse of the existing condition, gave her pain; but it effected a complete and permanent cure both of the squint and of the amblyopia. The same method has proved successful with other patients.
Some patients do not know whether they are looking straight at an object or not. These may be helped by watching the deviating eye and directing them to look more nearly in the proper direction. When the deviating eye looks directly at an object the strain to see is less, and the vision is consequently improved. Covering the good eye with an opaque screen, or with ground glass, encourages a more proper use of the squinting eye, especially if the vision of that eye is imperfect.
Children of six years, or younger, can usually be cured of squint by the use of atropine, a one per cent solution being instilled into one or both eyes twice a day, for many months, a year, or longer. The atropine makes it more difficult for the child to see, and makes the sunlight disagreeable. In order to overcome this handicap it has to relax, and the relaxation cures the squint.
The improvement resulting from eye education in cases of squint and amblyopia is sometimes so rapid as to be almost incredible. The following are a few of many other examples that might be quoted:
A girl of eleven had convergent vertical squint of the left eye. The vision of this eye at the distance was 3/200, while at the near-point it was so imperfect that she was unable to read. The vision of the right eye was normal both for the near-point and the distance. She was wearing glasses when she came to the office—convex 4.00 D. S. combined with convex 0.50 D. C., axis 90, for the right eye; and convex 5.50 D. S. for the left eye—but had obtained no benefit from them. When she looked three feet away from the big C with the left eye, she saw it better than when she looked directly at it; but when asked to count my fingers held three feet away from the card, they so attracted her attention that she was able to see the large letter worse. The fact was impressed upon her that she could see the card better when she looked away from it, or she could see it worse, at will; and she was also asked to note that when she saw it worse her vision improved, and when she saw it better her vision declined. After shifting from the card to a point three feet away from it, and seeing the former worse a few times, her vision improved to 10/200. The ability to shift and see worse improved by practice so rapidly that in less than ten days her vision was normal in both eyes, and in less than two weeks it had improved to 20/10, while diamond type was read with each eye at from three inches to twenty inches. In less than three weeks her vision for the distance was 20/5, by artificial light, and she read photographic type reductions at two inches, the tests being made with both eyes together and with each eye separately. She also read strange test cards as readily as the familiar ones. She was advised to continue the treatment at home to prevent a relapse, and at the end of three years none had occurred. During the treatment at the office and practice at home the good eye was covered with an opaque screen, but this was not worn at other times.
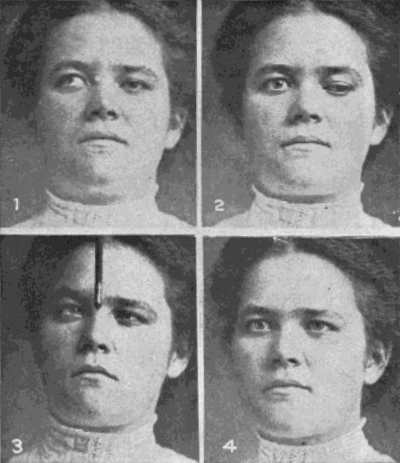
Fig. 54. Case of Divergent Vertical Squint Cured by Eye Education
No. 1.—The right eye turns out and up, the left being straight.
No. 2.—The patient learns to look down and out with the left eye while the right looks straight.
No. 3.—The patient learns to turn both eyes in by looking at a pencil held over the bridge of the nose.
No. 4.—The patient is permanently cured.
All four pictures were taken within fifteen minutes of each other, the patient having learned to reproduce the conditions represented at will.
A very remarkable case was that of a girl of fourteen who had squinted from childhood. The internal rectus of the right eye had been cut when she was two years old, but still pulled the eye inward. The patient objected to wearing a ground glass over her good eye, because her friends teased her about it and she thought it made her more conspicuous than the squint. One day she lost her glasses in the snow; but her father, who was a man of strong character, immediately provided another pair. Then she announced that she was ill, and couldn't go to school. I told the father that his daughter was hysterical, and simply imagined she was ill to avoid treatment. He insisted that she continue, and as she did not consider herself well enough to come to see me, I called upon her. With the assistance of her father she was made to understand that she would have to continue the treatment until she was cured, and she at once went to work with such energy and intelligence that in half an hour the vision of the squinting and amblyopic eye had improved from 3/200 to 20/30. She also became able to read fine print at twelve inches. She went back to school wearing the ground glass over the good eye; but whenever she wanted to see she looked over the top of it. Her father followed her to school, and insisted that she use the poorer eye instead of the better one. She became convinced that the simplest way out of her troubles would be to follow my instructions, and in less than a week the squint was corrected and she had perfect vision in both eyes. At the beginning of the treatment she could not count her fingers at three feet with the poorer eye, and in three weeks, including all the time that she wasted, she had perfect sight. When told that she was cured her main concern seemed to be to know whether she would have to wear the ground glass any more. She was assured that she would not have to do so unless there was a relapse, but there never was any relapse.1
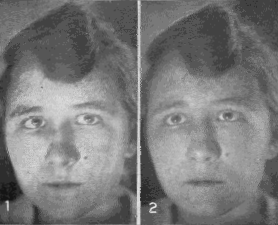
Fig. 55
No. 1.—Convergent squint of the right eye.
No. 2.—The patient is temporarily cured by the memory of a black period.
A girl of eight had had amblyopia and squint since childhood. The vision of the right eye was 10/40, while that of the left was 20/30. Glasses did not improve either eye. The patient was seated twenty feet from a Snellen test card and the right, or poorer eye, was covered with an opaque screen. She was directed to look with her better eye at the large letter on the card and to note its clearness. Next she was told to look at a point three feet to one side of the card, and her attention was called to the fact that she did not then see the large letter so well. The point of fixation was brought closer and closer to the letter, until she appreciated the fact that her vision was lowered when she looked only a few inches to one side of it. When she looked at a small letter she readily recognized that an eccentric fixation of less than an inch lowered the vision.
After she had learned to increase the amblyopia of the better eye, this eye was covered while she was taught how to lower the vision of the other, or poorer eye, by increasing its eccentric fixation. This was accomplished in a few minutes. She was told that the cause of her defective sight was her habit of looking at objects with a part of the retina to one side of the true center of sight. She was advised to see by looking straight at the Snellen card. In less than half an hour the vision of the left eye became normal, while the right improved from 10/l40 to 10/10. The cure was complete in two weeks.
The following case was unusually prolonged, because as soon as one eye had been cured the defect for which it had been treated appeared in the other eye. The patient, a child of ten, had imperfect sight in both eyes, but worse in the right than in the left. The vision of the right eye was restored after some weeks by eye education, when the left eye turned in and became amblyopic. The right eye was then covered, and after a few weeks of eye education the left became normal. The right eye then turned in and the vision became defective. It was necessary to educate the eyes alternately, for about a year, before both became normal at the same time. This patient had congenital paralysis of the external rectus muscle in both eyes, a condition which was apparently not relieved when the squint and amblyopia were cured.
In the following case the patient had an attack of infantile paralysis after her cure, resulting in a relapse, with new and more serious developments, which were, however, quickly cured. The patient, a girl of six, seen first on December 11, 1914, had had divergent squint of the left eye for three years, and had worn glasses for two years without benefit—convex 2.50 D. S. for the right eye, and convex 6.00 D. S. combined with convex 1.00 D. C., axis 90, for the left The vision of the right eye with glasses was 12/15 and of the left 12/200. Atropine was prescribed for the right eye for the purpose of partially blinding it and thus encouraging a more nearly proper use of the squinting eye, and the usual methods of securing relaxation, such as shifting, palming, the exercise of the memory, etc., were used. On January 13, 1915, the vision without glasses had improved to 10/70 for the right eye, and 10/50 for the left. On February 6, the vision of the right eye was 10/40 and of the left 10/30. The eyes were apparently straight, and scientific tests showed that both were used at the same time (binocular single vision). On April 17, after about four months' treatment, the vision of the left eye was normal, and there was binocular single vision at six inches. On May 1 the vision of the left eye was still normal, and whereas at the beginning the patient had been unable to read with it at all, even with glasses, she now read diamond type without glasses at six inches.
On August 16, 1916, the patient had an attack of infantile paralysis which was then epidemic. The sight of both eyes failed, the muscles that turned the eyes in and out were paralyzed, the eyelids twitched, and there was double vision. Various muscles of the head, the left leg and the left arm were also paralyzed. When she left the hospital after five weeks the left eye was turned in, and the vision of both eyes was so poor that she was unable to recognize her mother. Later she developed alternate convergent squint. On November 2 the paralysis in the right eye subsided, and four weeks later that of the left eye began to improve. On November 9 she returned for treatment without any conspicuous squint, but still suffering from double vision, with the images sometimes on the same side and sometimes on opposite sides. On November 23 the eyes were straight and the vision normal.
On July 11, 1918, the eyes were still straight and the vision normal, and there was binocular single vision at six inches. Although atropine had been used in the right eye every day for more than a year, and intermittently for a much longer time, and the pupil was dilated to the maximum, it read fine print without difficulty at six inches, central fixation overcoming the paralyzing effect of the drug. According to the current theory the accommodation should have been completely paralyzed, making near vision quite impossible. The patient also read fine print with the left eye as well as, or better than, with the right eye.
1. Bates: L'éducation de l'oeil dans l'amblyopie ex anopsia, Clin. Opht., Dec. 10, 1912.
| Уход за глазамиФизикаНаука БейтсаЛазер. коррек.Синя. под глаз.Зуд, жжения в глазахВраче. тайнаДр. болезни | |