




Better Eyesight
by William H. Bates, M. D. Д. Бейтс
Better Eyesight
A MONTHLY MAGAZINE DEVOTED TO THE PREVENTION AND CURE OF IMPERFECT SIGHT WITHOUT GLASSES
October, 1920
GO TO THE MOVIES
Cinematograph pictures are commonly supposed to be very injurious to the eyes, and it is a fact that they often cause much discomfort and lowering of vision. They can, however, be made a means of improving the sight. When they hurt the eyes it is because the subject strains to see them. If this tendency to strain can be overcome, the vision is always improved, and, if the practice of viewing the pictures is continued long enough, nearsight, astigmatism and other troubles are cured.
If your sight is imperfect, therefore, you will find it an advantage to go to the movies frequently and learn to look at the pictures without strain. If they hurt your eyes, look away to the dark for a while, then look at a corner of the picture; look away again, and then look a little nearer to the center; and so on. In this way you may soon become able to look directly at the picture without discomfort. If this does not help, try palming for five minutes or longer. Dodge the pain, in short, and prevent the eyestrain by constant shifting, or by palming.
If you become able to look at the movies without discomfort, nothing else will bother you.
THE PROBLEM OF IMPERFECT SIGHT
By W. H. Bates, M. D.
The problem of imperfect sight is such a tremendous one that few, even of those who specialize in such matters, realize its proportions, while outside this circle there is not the remotest conception of what it means.
The literature of the subject is very confusing and contradictory; but from the facts available there can be no doubt that the great majority of school children suffer from some degree of imperfect sight, while among adults normal vision is a rare exception.
The very careful investigation of Risley showed that in the public schools of Philadelphia, among children between eight and a half and seventeen and a half, the proportion of imperfect sight was about ninety per cent,1 other investigators report lower figures, but in many cases this simply means a lower standard. The findings of Risley agree with those obtained by myself in a study of 100,000 children made under all sorts of conditions in both city and country schools.
As to the sight of the adult population the operation of the draft law has supplied us with some unimpeachable data. It was found impossible to raise an army with even half normal vision in one eye, and in order to get the number of soldiers required it was necessary to accept for general service men whose vision could be brought up to half normal with glasses.2
Stich figures as the foregoing, terrible as they are, by no means exhaust the subject. In fact they are only the beginning.
Errors of refraction are so common that we have learned to take them lightly. They are usually reckoned among minor physical defects, and the average lay person has no idea of their real character. It is well known, of course, that they sometimes produce very serious nervous conditions, but the fact that they also lead to all sorts of eye diseases is known only to specialists, and not fully appreciated even by them. The complications of myopia (nearsight) constitute a large and melancholy chapter in the science of the eye, but most eye specialists say that no organic changes occur in hypermetropia (farsight). That this is very far from being the case was proven by Risley in the investigation alluded to above, and it is strange that his report on the subject has attracted so little attention. His studies also showed that these organic changes occurring in all states of refraction, are very common among children and have often progressed to an extent that would be expected only after long years of eyestrain.
In the case of myopic astigmatism the percentage of diseased eyes among all the children examined ran as high as eighty-seven per cent, and in the secondary schools not a single myopic eye was found with a healthy eyeground. The condition known as conus in which the choroid, or middle coat of the eye, is destroyed in the neighborhood of the optic nerve exposing the white outer coat (sclera) and forming first a crescent and later even a complete circle is commonly regarded as one of the symptoms of myopia and attributed to the tension resulting from the lengthening of the globe, but Risley's statistics show that while it is somewhat more common in this state of refraction than in hypermetropia it is by no means peculiar to it. In hypermetropia it was found in twenty per cent of the cases, and in hypermetropic astigmatism in forty-five per cent. In simple myopia it was present in forty-one per cent of the cases, and in myopic astigmatism it reached sixty per cent. It is a terrible thing to think that the eyes of our children should show a symptom of this character in such a large proportion of cases
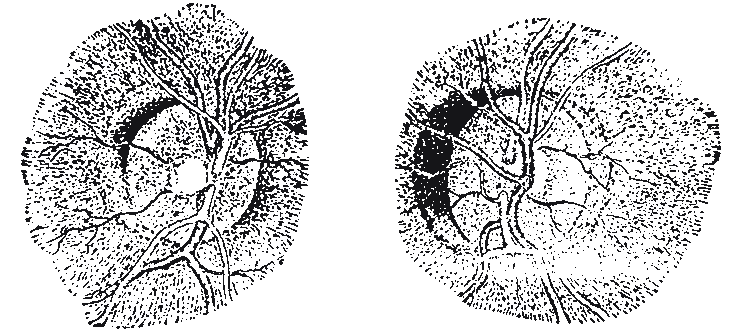
CONUS IN HYPERMETROPIA
The eyegrounds of a brother and sister aged respectively ten and twelve years. Both had hypemetropic astigmatism. "The conditions here represented," says Risley. "were repeated in scores of their fellows at school."
My own experience is that errors of refraction are always accompanied by some organic change. It may be only a slight congestion, but this may be sufficient to lower the vision.
By wearing glasses, avoiding poor lights and limiting the use of the eyes for near work, it is supposed that we can do something to prevent the development of these organic diseases and to check their progress; but for none of the traditional methods of treatment is it even claimed that they can be depended upon to preserve the sight as long as it may be needed, and Sidler Huguenin,in a paper several times referred to in this magazine, has stated that in the thousands of cases of myopia that have come under his observation they never were of any material benefit.3
That imperfect sight is a fruitful cause of retardation in school is well known. According to the New York City Board of Health it is responsible for a quarter of the habitually left backs.4 But that this condition cannot be remedied by glasses has not been generally observed. By making the patient more comfortable glasses do often improve his mental condition, but since they cannot relieve the mental strain that underlies the visual one, they cannot improve it to normal and by confirming it in a bad habit they may make it worse.
From the foregoing facts it will be seen that in the condition of the eyesight of our people we have a health problem, an educational problem, and a military problem, of the first magnitude, and one would think that if any method of either prevention or cure that was even tolerably successful had been found it would immediately be put into general use.
STORIES FROM THE CLINIC
8: Atrophy of the Optic Nerve
By Emily C. Lierman
About twenty-five years ago a patient came to the New York Eye Infirmary with well-marked atrophy of the optic nerve. According to all that we know of the laws of pathology he should have been totally blind; yet his vision was normal. The case was considered so remarkable that it was exhibited before a number of medical societies, but it was by no means an isolated one. On February 8, 1917, the editor published in the "New York Medical Journal," under the title, "Blindness Relieved By a New Method of Treatment," [link] a report of a case in which the vision was improved from perception of light to normal. He has had quite a number of such cases.
Some time ago a colored woman was led into the clinic by a friend. She had heard of Dr. Bates, and had come to him in the hope that he might be able to restore her sight. The doctor examined her eyes, and found that she had atrophy of the optic nerve complicated with other troubles. She could not count her fingers, nor had she any perception of light whatever. The doctor turned her over to me saying:
"Help her, will you?"
"She was the real "mammy" type of negro, very good-natured and motherly. She greeted me with a smile and said:
"May de good Lot' bless you, ma'am, of you can gives me again de light ob day."
The words came from a very humble heart, and were very hopeful. When I heard them I can tell you that I lost some of my courage. It might turn out that I could do nothing for her, and I dreaded to disappoint her. My work is not always easy; yet I like the hard cases to come my way, because when I can help them I feel that I have done something worth while.
"Won't you tell me how long you have been blind?" I asked.
"Yes, ma'am," she replied. "I's hasn't seed nothin' for two years, I's been in the hospital all dat time an' de doctors says dat mebbe I's nebber see again. Some friend ob mine says to me, `You jes goes to de Harlem Hospital Clinic. Dere you find de doctor what makes you see.' So I jes come; dat's all."
I told her to cover her eyes with the palms of her hands and asked if she could remember anything black. She replied
"Yes, ma'am, I 'member stove polish black, all right." "That's fine," I said. "Now, keep remembering the black stove polish, and that will stop the strain in your eyes. When your eyes first began to trouble you, you strained to see, and every time you did that your eyes became worse. Now let us see what will happen when you stop the strain." I stood her against the wall to make things easier for her, for we have few chairs at the clinic, and left her to treat other patients, telling her not to open her eyes, nor to remove her palms from them, not for a moment, till I came back. Presently I became aware of a strange sound, a sort of mumbling. I was greatly puzzled, but tried not to show it for fear I would disturb the patients. All of a sudden, as I approached my blind patient, I discovered where the sound came from. She was saying in a low tone, "Black polish, black polish," just as fast as she could. I now held a test card covered with E's of various sizes turned in different directions a foot away from her eyes, and told her to take her hands down and look at it. The doctor, the other patients and myself were quite scared at the outburst that followed.
"Ma'am, dat's a E; dat's a sure-nough E. I's sure dat's a black E on some white paper."
This was a large letter on the first line, read by the normal eye at two hundred feet.
But the next moment it faded from her eyes. That was my fault. I was not quick enough. What I should have done was to have her close her eyes and palm again the moment she saw the E. But I was greatly encouraged, not only because the patient had had a flash of vision, but because Dr. Bates had said he was sure I would help her to see again. I again told her to palm and remember black, and when, in a few moments, I asked her to take down her hands and look at the card, she again saw the E, and blacker than the first time. I now told her to close her eyes for a minute and open them for just a second, alternately, remembering the stove polish as she did so. She did this for a time, and was able to see the E each time she opened her eyes.
"Now," I said, as I raised my hand and held it one foot from her eyes, "how many fingers can you see?" "Three," she replied, which was correct.
I told her to rest her eyes by palming many times a day, and to come and see me three times a week. I also gave her some advice about her diet, and told her that enemas were quite necessary to relieve her constipation.
Next clinic day she saw the seventy line of letters at one foot, and they did not fade away as did the E the first time she saw it. I told her to palm some more, and in a few minutes she counted my fingers correctly every time I asked her to, with only one exception.
"If dis here seein' keeps up, ma'am," she remarked, "I sure will be able to earn mar livin' again. De Lor' bless you ma'am."
She continued to come and made slow but sure progress for a time. Then came a time when she stayed away for several months. As I was very anxious to cure her, I worried about her considerably during this time. Then one day she turned up again. She seemed to be very much frightened about something, but her eyes looked much better. I was so glad to see her, and she seemed so much upset, that I refrained from scolding her, as I felt like doing, and in course of time I discovered the reason for her absence. She had been under treatment for some other troubles, and some doctor or nurse had scared her into discontinuing her visits to our clinic. She had, however, continued to palm several hours a day with most gratifying results.
"Do you know, ma'am," she said, "I's can see every house number as I go visitin', an' I goes out to a day's work once in a while."
She continued to come quite regularly, and her improvement continued. Sometimes I would find that she did not see as well as at her previous visit, but immediate improvement always followed palming. Her gratitude was pathetic, and every little while she would bring a bundle, saying:
"Dis here is fo' you, ma'am. You sabe me from blindness. Yes, you did, an' I's mighty grateful."
These bundles contained gifts of various kinds—a cocoanut from the West Indies at one time, grapefruit and cucumbers at another, and a third a necklace made of tropical beans of various colors.
The greatest day of her life came a few weeks ago when she washed a full set of Dresden china for her employer, without breaking a single piece, and earned four dollars and twenty cents by her day's work. If she continues to practice the palming, which she now forgets sometimes, I have no doubt that she will, in time, obtain normal vision. She now sees the largest letter on the card twenty feet away, and reads the headlines in the newspapers. Recently Dr. Bates examined her eyes with the ophthalmoscope, and found the appearance of the optic nerve very much improved, more blood-vessels being visible in the papilla, or head of the nerve.
HOW I LEARNED TO SEE
By Irma Meyers
This patient was fourteen years old when first seen, and was wearing the following glasses: Right eye, concave 3.12 D. S. combined with concave 0.75 D. C., 90 degrees; left eye, concave 3.25 D. S. combined with concave 0.50 D. C., 90 degrees. At the second treatment her sight had improved temporarily to 20/20, and at the third she had a flash of perfect sight.
The time had come for me to consult an oculist again. I had been wearing glasses far over a year, and they had always been a torment to my parents.
We were discussing the question of oculists at table. My father contended that if there were physicians who could correct defective sight with glasses, there must be those who could cure such defects so that glasses would not be necessary. He had heard of a Dr. Bates who had cured people so that they no longer had to wear glasses.
So instead of going to an eye specialist who would probably have prescribed new glasses, father and I went to see Dr. Bates. While waiting for admission to his private office a number of questions came to my mind. Could he cure me? Would I be able to get along without glasses for the rest of my life? It seemed too good to be true. My eyesight had been so poor that I had given up hope of ever leaving off my glasses.
Finally we were ushered into Dr. Bates' office. He examined my eyes. I could just barely read the second line of letters on the Snellen chart—which shows bow defective my eyesight was. The doctor impressed upon me that to improve my sight depended largely upon myself, and I determined to follow his directions conscientiously. I must never wear my glasses again, I was told, and that day, in the doctor's office, was the last time I did wear those hated glasses.
Then the doctor told me to palm—that is, to put my hands over my eyes in such a way as to exclude all the light from them. In this way my eyes became rested. I was not looking at anything, and therefore my eyes were not undergoing any strain. Next the doctor showed me some fine print on a card and called my attention to the fact that while these letters looked perfectly black to me, those on the Suellen chart, at a distance of ten feet, were gray. The difference was due to my imagination, he said, and proved that my eyesight was not normal, because the letters on the test card were just as black as those on the small card in my hand. Then he told me how to improve my imagination. In reading letters like O, D, and S, which had open spaces in them, I was to imagine the white openings (the card is white, the letters black) whiter than the margin of the card, which is the way the normal eye sees them. When I became able to do this the black letters stood out more clearly.
Besides my imagination I had also to exercise my memory. This was accomplished in this way: I looked at a certain letter on the chart. Then I closed my eyes and remembered it better than I saw it. I could not do this very well at first, but my memory improved with practice.
These and many other methods of improving the sight I learned from Dr. Bates. I visited him three times each week, and soon began to read much more on the chart than I had at my first visit. At the same time I noticed that stores, signs, houses, cars, all material objects, began to come out more clearly than before. I discovered, too, that I was not so shaky on my feet as I had been when I first discarded my eyeglasses. I felt then as if I would fall at every step I took . In school I did not have to go up to the blackboard to read what was on it, and did not have to sit as near the front as I formerly did.
After six or seven months I began to enjoy the movies. I no longer had to sit and view a picture that I could not see. (I never, as I said before, used my glasses after my first visit to Dr. Bates.) I began to enjoy the pictures as much as the people around me who had never worn glasses. In school I could sit in the last rows and read the blackboard without any trouble.
I have now been under treatment about a year, with some interruptions, and my eyesight is considered normal. At a recent test by the visiting physician at school I stood second among forty odd pupils. The girl who was first read just one letter more than I did, and I am sure that if I had had an opportunity to palm I would have been able to do better than she did.
I cannot express in words what I owe to Dr. Bates. I shall always be grateful to him, and I wish I could show my appreciation for his work.
At a recent visit Dr. Bates told me that my cure was not yet permanent, but I shall continue to follow his instructions and teachings implicitly until it is permanent. I sincerely hope that I shall never go back to wearing glasses, and that this recital of my experiences may help others similarly afflicted.
QUESTIONS AND ANSWERS
All readers of this magazine are invited to send questions to the editor regarding any difficulties they may experience in using the various methods of treatment which it recommends. These will be answered as promptly as possible. Kindly enclose a stamped addressed envelope.
Q. 1. When objects at a distance clear up they are double. Can you suggest a remedy for this double vision? 2. When I open my eyes after palming my sight gradually clears, but an intense pain often comes in my eyes, so that they close. The pain always starts with very clear vision. Is this eyestrain?—H. M.
A. 1. If the objects are double when they clear up, relaxation is not complete, and the only remedy is to secure a greater degree of relaxation. This may be done in many ways. Use the method you have found most effective. 2. Yes. Your sight should be best when you open your eyes. If it clears up afterward, it is because you are making an effort to see. This produces the pain.
Q. 1. How long should one palm and how often? 2. How young a patient can you treat by this method, and up to what age can you expect results? How would you handle a child that did not know its letters? 3. Is astigmatism curable by this method? 4. How long has the method?—J. H. W.
A. 1. As often and as long as possible. 2. The age is immaterial. It is a matter of intelligence. Patients as old as eighty-two have been relieved. Children can be treated as soon as they are able to talk. Any small object can be used for eye training, and in the case of children who do not know their letters, kindergarten and Montessori equipment is often useful. 3. Yes. 4. Its evolution began thirty-five years ago. It has improved as experience was gained, and is still improving.
1. Shool Hygiene, System of Diseases of the Eye, edited by Norris and Oliver.
2. Report of the Provost Marshal General to the Secretary of War on the First Draft under the Selective Service Act, 1917.
Second Report of the Provost Marshal General to the Secretary of War on the Operations of the Selective Service System to December 20, 1918.
3. School Health News, February, 1919.
4. Archiv. f. Augenh, vol. IXXIX, 1915, translated in Arch. Ophth., vol. XLV, Nov. 1916.
| Уход за глазамиФизикаНаука БейтсаЛазер. коррек.Синя. под глаз.Зуд, жжения в глазахВраче. тайнаДр. болезни | |